
Table of Contents
Name of Procedure
- Stellate ganglion block (SGB)
- Stellate sympathetic block
Sample Opnote
Goal
To administer medications around the stellate ganglion and cervical sympathetic trunk/chain.
Indications
Various chronic pain syndromes that are sympathetically mediated such as:
- Complex regional pain syndrome (CRPS)
- Ischemia induced pain in an upper extremity
It may have a role for a variety of other conditions as well:
- Phantom limb
- Atypical chest pain
- Intractable angina
- Refractory cardiac arrhythmias
- Hyperhidrosis
- Many others. See references for a more complete list.
Contraindications
- Common contraindications
- Blood thinners – See ASRA based guidelines (and an abbreviated protocol) for managing various blood thinners pre and post procedure
- Heart block or bradycardia
- Contralateral diaphragmatic paralysis
- As seen in the anatomy you’ll probably get an ipsilateral phrenic nerve block while doing this procedure, which could theoretically result in transient ipsilateral diaphragmatic weakness. If the contralateral diaphragm suffers from any dysfunction this could cause temporary respiratory failure after the block.
Anatomy
Overview
The stellate ganglion:
- Is a combination of the inferior cervical ganglion and 1st thoracic ganglion
- Should sit just anterior to the C7 transverse process
- Has postganglionic fibers that go to the arms, head and neck, along with some innervation to the heart
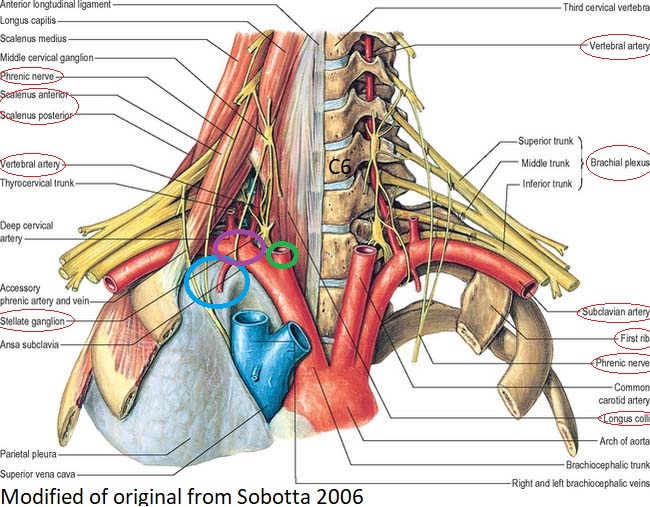
Anatomy of stellate ganglion and related structures. Circled labels particularly important for the procedure. Blue circle lung pleura. Purple circle subclavian artery. Green circle carotid artery.
Structures
- Borders:
- longus colli muscle medially (red)
- scalenes laterally (red)
- subclavian artery anteriorly (purple circle)
- transverse processes posteriorly
- pleura inferiorly (blue circle)
- carotid artery anteriorly (green circle)
- Nearby:
- phrenic nerve (red)
- recurrent laryngeal nerve
- the brachial plexus (red)
NOTE: there is significant variation in the ganglion’s composition and location:
- Only present in 80% of the population. So in people without the ganglion, you may just be blocking the lower cervical and upper thoracic sympathetic nerves.
- Many patients have fibers of Kuntz that bypass the stellate ganglion and directly innervate the extremities, so a successful block of the ganglion may still fail to provide the desired effect.
Procedure Target
NOTE: the classic target is near the C6 transverse process (Chassaignac’s tubercle):
- The vertebral artery is posterior to the transverse processes at C6, but at C7 it runs anteriorly.
- Therefore if your needle tip is at C6, there might be a lower risk of vertebral artery vascular uptake.
- The higher target at C6 may also help avoid pleural lung puncture.
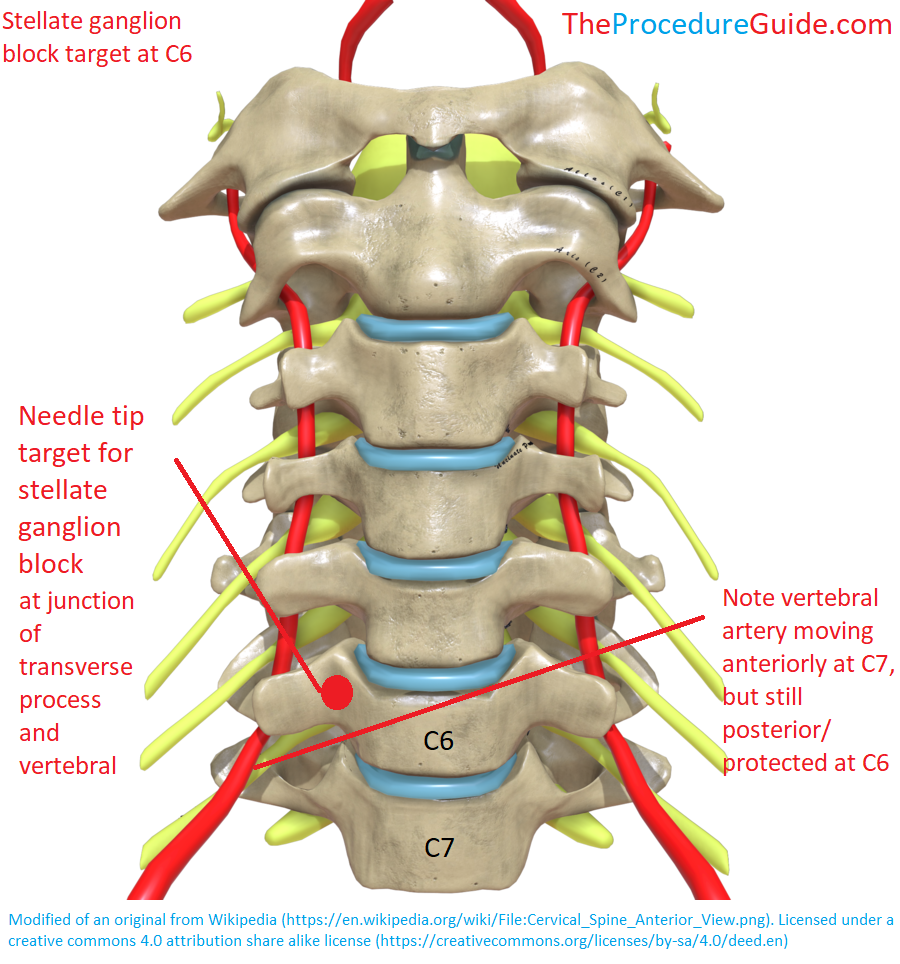
Stellate ganglion injection target at C6 and relationship to vertebral artery.
Equipment/Skills/Setup
Equipment
- Steroid and/or local anesthetic injectate
- 25 gauge spinal needle
- A 25g needle might reduce the risk of bleeding in the event of inadvertent puncture of a vascular structure.
- 2-3cc contrast
- Short, low volume tubing
- To attach after needle placement to inject through
- Be sure to prime the tubing so there isn’t any air.
Prep
Adverse reactions or complications could be severe and require emergent management. Therefore a preoperative IV may be useful.
Landmarks and Patient Positioning
Basic supine position with the neck in an extended position so that you have good access to the anterior neck.
Technique
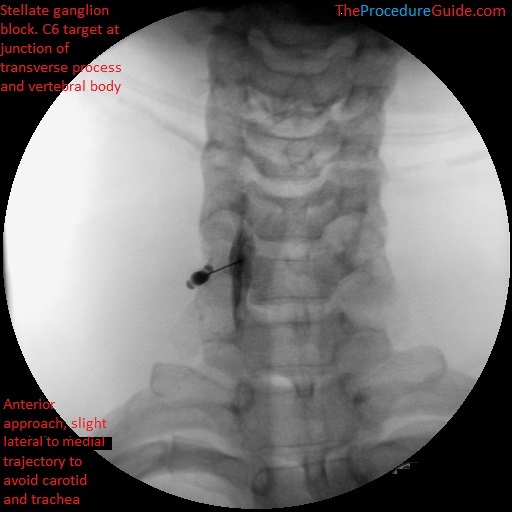
Stellate ganglion block with contrast at C6 under fluoroscopy
- Obtain an AP view and identify C6
- Identify the first rib to see T12 and count up from there. Alternatively, count from the top: Tilt the c-arm to match the cervical curvature so you can count one level at a time.
- Level off C6
- Use a pointer to identify a spot just superficial to your target
- Palpate the carotid artery and trachea
- Try to apply traction laterally on the carotid
- Insert your needle
- You can mostly try for a “down the barrel” approach so you enter right above your target
- The trachea may be in the way so you may start slightly lateral (but medial to the carotid) and aim medially towards your target (as seen in the image below).
- If you always keep the needle above bone then you know that you will have to hit bone before going too deep.
- Contact your target
- Lift the needle tip off the bone slightly
- Consider attaching a PRIMED (NO air) short, low volume tubing:
- This helps keep the needle tip steady during aspiration/injection
- Allows live contrast injection with your hands away from the field of view
- Aspirate first and perhaps at various points during the injection to ensure that you don’t get air or blood.
- Inject desired medication slowly
Risks and Complications
This procedure has a uniquely large number of potentially serious complications. Note some technique points that help mitigate these:
- Puncture/bleeding from any number of vascular structures: carotid artery, subclavian artery, jugular vein, vertebral artery.
- Several attempts at aspiration and live contrast injection
- Palpation over the carotid to keep the needle away from that vessel.
- Pneumothorax via puncture of the apex of the lung
- Aspiration to check for air. Small gauge needle to potentially reduce the likelihood of symptomatic puncture.
- C6 target, which is further from the lung.
- Vertebral artery injection
- C6 as a target site, frequent aspiration, and live fluoro injection.
- Radicular nerve root injury or involvement
- Anterior approach “down the barrel”, bony contact on the anterior surface of the transverse process/body, and proper contrast spread.
- Emergent complications:
- Any of the above can result in an emergency. A preoperative IV will help with quick vascular access if needed.
- Avoid an overly quick discharge from PACU.
References
Procedure
- Dr. Nur Surya Wirawan – Stellate Ganglion Block ISAPM 2015
- Very good slide review of various stellate ganglion block techniques.
- Stellate Ganglion Blocks – StatPearls – NCBI Bookshelf
- Thorough list of indications and procedural steps
- How I Do It: Stellate Ganglion Blocks
- Ultrasound images
- Stellate Ganglion Block Anaesthesia Tutorial Of The Week 256 : Wfsa – Resources
- Tips for blind vs fluoro vs CT vs US guided
General
- Stellate ganglion block: effects
- Sonographic Nerve Tracking in the Cervical Region: A Pictorial Essay and Video Demonstration
- Cervical nerve tracking technique
- Cervical Sympathetic Trunk| Superior, Middle & Inferior Ganglia| Situations | Relations | Branches
- Detailed review of the cervical sympathetic chain