
Table of Contents
Name of Procedure
- Genicular Nerve Block Radiofrequency Ablation
- Neurotomy, rhizotomy, “nerve burn”, RFA
💰 Medicare Data Explorer and Calculator
See payment rates and wRVUs from public CMS data. And use our calculator to model procedures and your practice.
Explore data for a Genicular Nerve Radiofrequency Ablation →
Sample Opnote
Goal
To ablate the genicular nerves that innervate the knee to provide long term relief of pain in the knee.
Indications
A genicular nerve radiofrequency ablation is used to treat pain from the knee from a variety of causes. It has the benefit of treating many causes such as arthritis, intraarticular pathology and even pain in patients who have had prior surgery or total and partial knee replacements.
This makes the procedure an option when intra articular treatments such as a knee steroid or hyaluronic acid injection isn’t an option.
A diagnostic genicular nerve block might help inform if a radiofrequency ablation of the genicular nerves should be performed for the patient.
Contraindications
Anatomy
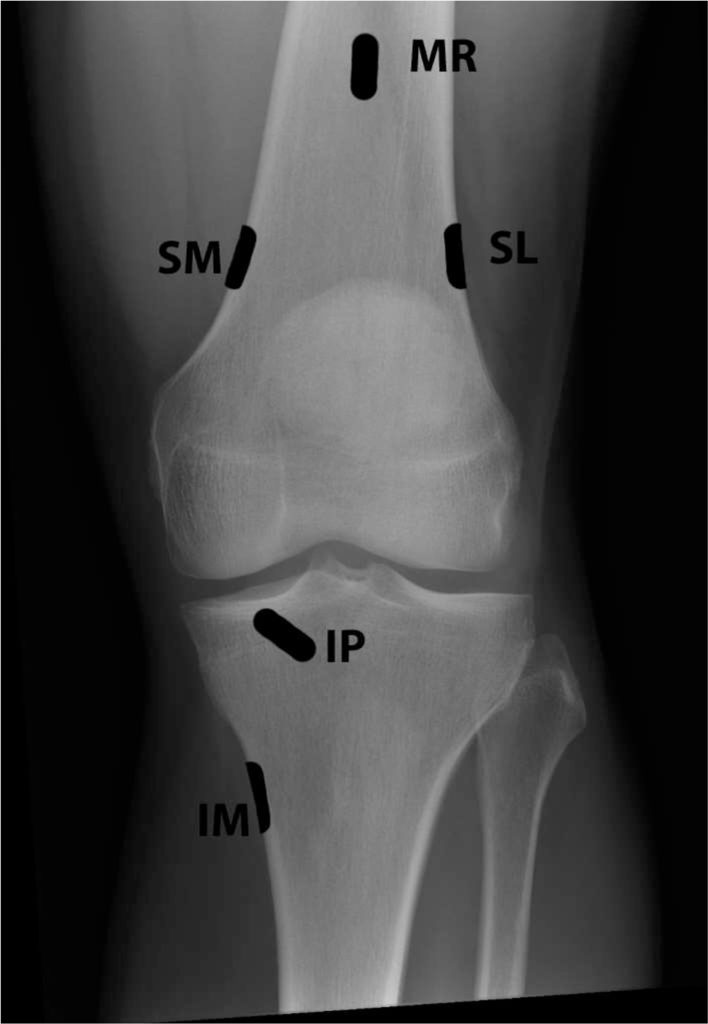
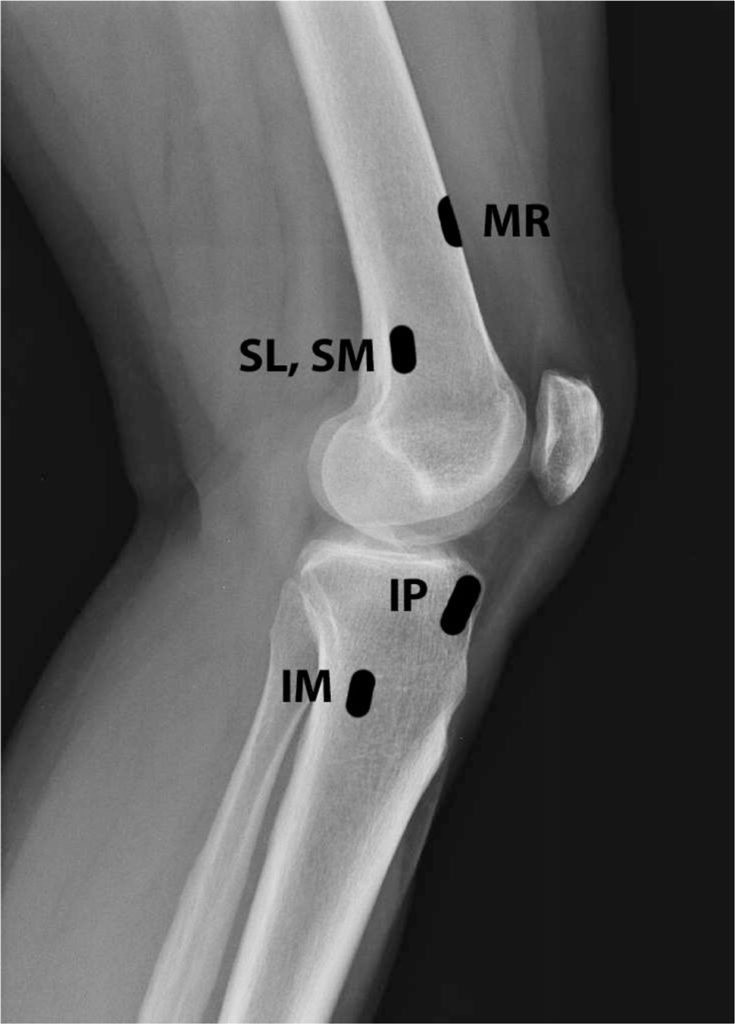
The knee is innervated by several genicular nerves. These nerves are articular branches formed from the femoral, saphenous, common peroneal, tibial and obturator nerves. There are several branches, but the following 3 are the ones targeted for treatment. They run along the bones, which give us fluoro targets:
- Superior lateral (SL) (along femur)
- Superior medial (SM) (along femur)
- Inferior medial (IM) (along tibia)
Equipment/Skills/Setup
Core Equipment/Disposables: See our disposables/equipment article for “core” items that are common to all procedures.
Special items and suggested setup for this procedure (see quick guide video above for example tray prep):
- RF cannula and probe with RF machine. (2 cannulas and 1 probe will allow for placement of a second cannula, while the prior one is ablating)
- 3cc 1% lidocaine in 3cc syringe
- 10cc 1% lidocaine in 10cc syringe with 25g x 1.5″ hypodermic needle for subcutaneous anesthetic
Landmarks and Patient Positioning
- Position the patient in a basic supine position.
- Bend the operative leg to about 45 degrees or a little less and keep the contralateral leg straight. (The goal is just to keep the non-operative leg out of the way while getting a lateral view)
- Alternatively you could bend the non-operative leg and keep the operative leg flat.
- Position the patient/bed so that the bottom of the c-arm can go under the table below the knee, then simply rotate for a lateral view of the knee.
Technique
Overview
As with other RF procedures, this technique tries to get the needle to “lay flat” against the bone to try and maximize the coverage area of the probe.
Here is your target and entry point [See our general guide about basics for using targets and entry points to start a procedure]:
- Target: As seen in the anatomy images above. We place our needles a bit more anterior on the femur than the diagram.
- Entry: Just above/anterior to the target
Steps
- Start with an AP view of the knee and place a pointer right over your first target: either the lateral or medial femoral targets (SM and SL in the diagram above).
- You’ll enter just barely lateral to the bone so the needle runs alongside the bone while traveling posterior.
- Anesthetize, then insert the RF cannula and attempt to contact bone at the antero-lateral edge.
- Switch to a lateral view
- Continue to advance the needle along the bone in this view while injecting ~3cc lidocaine along the bone.
- You can adjust the cannula trajectory to have the tip sit over your final target.
- Ablate here
- Repeat the above steps for the other two target sites (SL, SM, IM targets in total)
Tips
- With 2 cannulas you can get a second cannula placed by the time the first cannula finishes it’s ablation.
References
Procedure Related
- Radiofrequency techniques to treat chronic knee pain: a comprehensive review of anatomy, effectiveness, treatment parameters, and patient selection
- Broad overview of many topics related to knee pain and RF in the pain literate.
- Good review of knee neuroanatomy
- Reviews many studies about RF for the knee and summarizes different RF modalities used in different studies along with their results.
- Prospective, Multicenter, Randomized, Crossover Clinical Trial Comparing the Safety and Effectiveness of Cooled Radiofrequency Ablation With Corticosteroid Injection in the Management of Knee Pain From Osteoarthritis
- Reviews some technique and has images for genicular block and RF.
General Clinical
- Radiofrequency treatment relieves chronic knee osteoarthritis pain: a double-blind randomized controlled trial
- Kim SY, Le PU, Kosharskyy B, et al. Is genicular nerve radiofrequency ablation safe? A literature review and anatomical study. Pain Physician. 2016;19(5):E697–E705. [PubMed] [Google Scholar]
- Davis T, Loudermilk E, Depalma M, et al. Prospective, multicenter, randomized, crossover clinical trial comparing the safety and effectiveness of cooled radiofrequency ablation with corticosteroid injection in the management of knee pain from osteoarthritis. Reg Anesth Pain Med. 2018;43(1):84–91. [PMC free article] [PubMed] [Google Scholar]
- Qudsi-Sinclair S, Borrás-Rubio E, Abellan-Guillén JF, Padilla del Rey ML, Ruiz-Merino G. A comparison of genicular nerve treatment using either radiofrequency or analgesic block with corticosteroid for pain after a total knee arthroplasty: a double-blind, randomized clinical study. Pain Pract. 2017;17(5):578–588. [PubMed] [Google Scholar]
- Hirasawa Y, Okajima S, Ohta M, Tokioka T. Nerve distribution to the human knee joint: anatomical and immunohistochemical study. Int Orthop. 2000;24(1):1–4. [PMC free article] [PubMed] [Google Scholar]
- Kennedy JC, Alexander IJ, Hayes KC. Nerve supply of the human knee and its functional importance. Am J Sports Med. 1982;10(6):329–335. [PubMed] [Google Scholar]
- Choi WJ, Hwang SJ, Song JG, et al. Radiofrequency treatment relieves chronic knee osteoarthritis pain: a double-blind randomized controlled trial. Pain. 2011;152(3):481–487. [PubMed] [Google Scholar]
- Sarı S, Aydın ON, Turan Y, et al. Which one is more effective for the clinical treatment of chronic pain in knee osteoarthritis: radiofrequency neurotomy of the genicular nerves or intra-articular injection? Int J Rheum Dis. 2016 Aug 12; Epub. [PubMed] [Google Scholar]
- Lindquist J, Bäckryd E. Pulsed radiofrequency in clinical practice – a retrospective analysis of 238 patients with chronic non-cancer pain treated at an academic tertiary pain centre. Scand J Pain. 2016;12:68–73. [PubMed] [Google Scholar]