
Table of Contents
Name of Procedure
Greater trochanteric bursa injection (with or without steroid) with fluoroscopy
Sample Opnote
Goal
To inject a medication into the greater trochanteric bursa
Indications
Depending on what’s injected, usually it is to treat pain from bursitis (greater trochanter pain syndrome)
Contraindications
Anatomy
For the purposes of hip injections, anatomy is straightforward.
- For an intraarticular injection:
- The anterior or lateral border of the femoral neck provides a good target for the needle tip (blue dot)
- Ideally the contrast will spread around the neck such as near the junction of the head and neck (purple line)
- The hip/upper femur have several bursae so we are going to focus on ones just lateral to the greater trochanter.
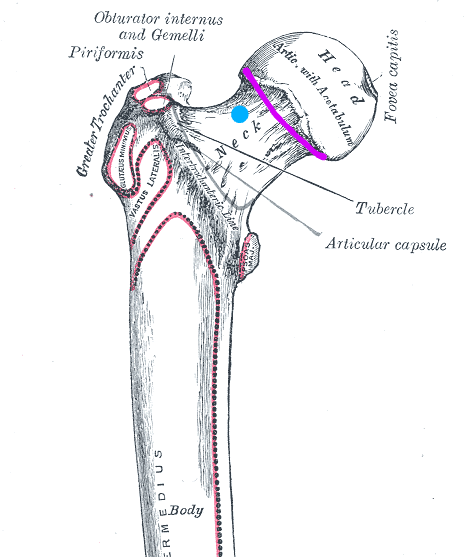
diagram of hip joint with target for needle for intraarticular injection and desired contrast spread. Modified of original at: https://commons.wikimedia.org/wiki/File:Gray244.png
Equipment/Skills
- C-Arm
- Bed for C-Arm
- 25g x 1.5″ hypodermic needle
- Contrast in 3cc syringe
- Desired injectate in 3cc syringe:
- bupivacaine/lidocaine
- steroid (dexamethasone/triamcinolone)
- prep solution
- drape to keep injection site clean
Landmarks and Patient Positioning
Position the patient in a basic supine position so that the bottom of the c-arm can go under the table below the hip.
Technique
Find your entry point:
- Assume your needle is entering from the lateral part of the thigh and aiming medially: In an AP view you do not have a good sense of where your needle is in an anterior-posterior direction/frontal plane (ie, it’s depth):
- If you check a lateral, unless both legs are perfectly aligned, it might be hard to know your needle depth in the anterior/posterior direction.
- Also, a lateral usually isn’t necessary: Feel the lateral thigh to assess where the femur is. This tells you your entry point and trajectory in the frontal plane.
- This is a complicated way of saying: feel the leg for the greater trochanter (marked below). This red line is the frontal plane that you want to keep your needle in while you’re advancing medial to hit the femoral neck.
Start your procedure:
- Get an AP view so that you see the greater trochanter and the skin in one view.
- Insert your 25g hypodermic needle towards the greater trochanter (staying in that frontal/red plane noted above).
- Contact bone near the middle or top of the trochanter then pull back slightly off the bone.
- Inject contrast.
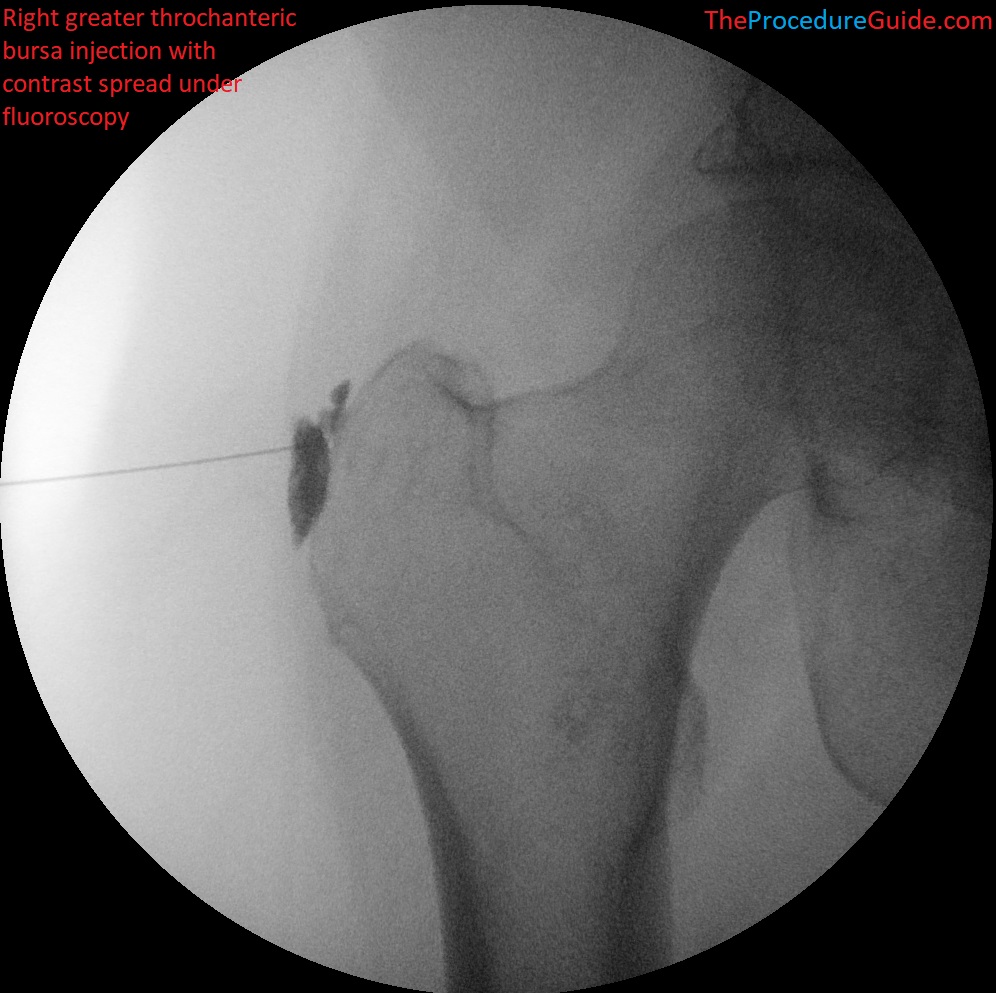
Greater trochanteric bursa injection with contrast under fluoroscopy
- You might need to reposition the needle to get ideal spread.
- Once in place simply inject your desired medication (such as 0.5% bupivacaine and 40mg triamcinolone, ~5cc).
Tips
- Usually a 25g x 1.5″ hypodermic needle is sufficient to reach your target.
- With this approach no second/larger needle is needed, and usually it can be done without subcutaneous/local anesthetic since it’s the 25g needle is the same one that would be used to administer local anesthetic anyway.
- If it turns out that the hypodermic needle is not long enough, just inject lidocaine through it while pulling out.
- Then use a longer needle such as a bent quincke needle to reach the joint space.
References
- Trochanteric Bursitis (Greater Trochanteric Pain Syndrome)
- Great overview of the entire syndrome including presentation, epidemiology, anatomy, differential, treatment options, etc.
- Home training, local corticosteroid injection, or radial shock wave therapy for greater trochanter pain syndrome
- Some review of the role for injections
- The occasional injection for trochanteric bursitis
- Some review of a blind technique and anatomy